This Assam Mechanic Made A 'Jugaad' Helicopter Using SUV Engines & Car Seats! Chandra Siwakoti Sharma recently built a jugaad helicopter using car seats and two SUV engines and guess what he named it? “Pawan Putra!” An automobile mechanic by profession, Sharma spent over rupees 15 lakhs from his own savings to design the unique invention. A resident of Shyamjuli village in Assam, Sharma dropped out of school after third grade due to poor financial conditions. But determination drove the man like no other. He used all his savings and even sold his land to build his Pawan Putra, an invention that's awaiting clearance from authorities.” February, 2016; Indiatimes.
This was an inspiring piece of news! It made us wonder, of somebody, who could innovate under such dire circumstances. What is amazing about the article is that Mr. Sharma, invented this, “Jugaad” helicopter to address poor transportation conditions at his village! This is a game changer... from, “no roads” to, “no need of roads!”
Working with the biological and pharmaceutical manufacturing industry, we have come across, some of the most wonderful organizations, where innovation is nurtured and encouraged. However, we have not seen many Chandra Siwakoti Sharmas’ at our shop-floor.
We have been some part of several culture change Initiatives, in the pharmaceutical and biological manufacturing organizations, and have seen our share of successes and failures, in the spaces that we have worked. When we look back and ponder on The Most Important Factor for a successful cultural transformation in the organizations, we could not come up with anything else but “the innovative implementation” of a very obvious solution to a herculean, or seeming herculean problem.
Inspired from Mr. Sharma’s tryst with, “no roads” to, “no need of roads” we decided to catalogue our experiences of critical pre-conditions, those need to be present or are required to be developed before a cultural transformation takes place!
While doing so we have taken a case of two similar sized multi-locational pharmaceutical organizations, and who had more or less the same aspirations of cultural transformation. Our time and nature of involvement with both the organizations was also very similar, approximately lasting four months. The work done at both the organizations was more than five years back and thus gives us benefit of assessing the outcome fairly. Needless to say, one organization is a phenomenal success today and other is still, “work in progress”.
We are bound by the confidentiality agreements with both the organizations, and hence will not delve more into the type of work we did with them and the nature and extent of the problem. However, for understanding of the reader of this article, the nature of the problem was, “workforce need to adhere to the standard procedures” or standardization of work processes at shop-floor. For our easy understanding we will name these organizations as “Success” and “work in progress”.
To provide more perspective, both organizations were able to achieve work process standardization at the location/operation, which they were targeting. However, the “success” organization was not only able to transfer the knowledge to other locations, without involving external help, but also was able to improve, on the initial work which was done, to make their processes robust and compliant.
The “work in progress” organization, although were able to achieve their targets then, but were unable to cascade the learning, either from one operation to other similar operations or take the learning into other locations. No further improvements were undertaken by this organization on the work processes. Therefore, it required and still requires constant support to solve similar problems at other locations.
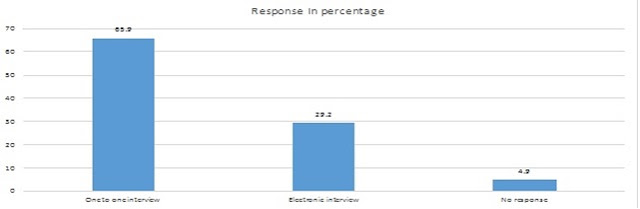
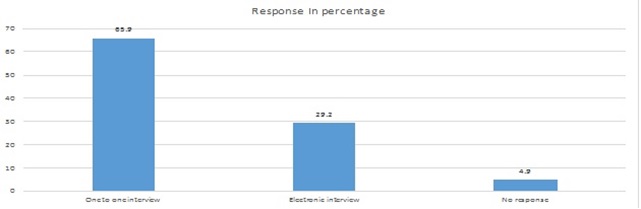
After reading the article on “Jugaad helicopter”, a review of the progress at both the organizations saw the authors spending two months, at the shop-floors of the original manufacturing locations. There were multiple interviews of the shop-floor personnel, managers and senior leadership, across both the organizations. The groups were divided into the following:
1.0 Those who were part of original four-month initiative, a total of 80 shop-floor personnel, 12 managers and 4 leaders.
2.0 Those who joined later in the same department, where original initiative was conducted. A total of 43 shop-floor personnel, 2 managers.
3.0 Other personnel and managers from other departments or locations. A total of 657 shop-floor personnel and 20 managers.
The study also accounted for the attrition in both the organizations; efforts were made to trace and interview the ex-employees; details are depicted in the graph below:
In the following section of this article, we will list and analyze the aspects, those which triggered or hampered, “innovative implementation” at these two organization.
Organization culture, which is conducive of innovation, is characterized with its ability to transform ideas quickly into experiments. These experiments can result in data, which is used for decision making for future change, implemented successfully. This can be divided into following stages:
1.0 Understanding the problem: Significant effort is made to understand the problem/opportunity, before taking next steps, instead of, “knee jerk” action.
2.0 Trust: People are able to experiment with ideas, without fear of backlash.
3.0 Zeal/ Inspiring curiosity: Focus is on What, Why and How, instead of “who”
4.0 Challenge current perspective and not averse to Risk: Processes and perception are put to scientific enquiry, instead of a general attitude of “not rocking the boat”.
5.0 Skill development by fostering partnership: Give and take is deep rooted and employees understand with every, “give” to someone, they are, “taking” a lot of experience.
6.0 Creating freedom and open dialogue: Employees/teams do not wait for right opportunity to speak on issues, rather anyone can discuss their issues, and seek solutions across the length and breadth of the organization.
7.0 Driving discipline/ criticism: Teams/Employees/managers do not feel offended, when feedback is provided, instead seek constructive criticism regularly.
We designed an experiment, to understand the underlying causes of transformation/ or lack of it in both the organizations. Through using tools, the data that emerged is represented below:

As depicted in the graph, the participant from, “success organization” gave higher ratings than, “Work in Progress organization”. This leads to quick implementation of learning, taken by one section/department to the entire organization. The higher ratings in one organization, do indicate a relation between their success and their culture of sustaining “innovative implementation”, when we compare it with the other organization.
However, this brings us to next question, how was one organization able to have all parameters ticked in for sustaining this learnt innovation despite the overall experience, the sizes, scale and challenges of both organizations being similar? We will discuss in the subsequent part of this article….In the meanwhile, if you wish to reach us, please do so at vienni.india@gmail.com.
This was an inspiring piece of news! It made us wonder, of somebody, who could innovate under such dire circumstances. What is amazing about the article is that Mr. Sharma, invented this, “Jugaad” helicopter to address poor transportation conditions at his village! This is a game changer... from, “no roads” to, “no need of roads!”
Working with the biological and pharmaceutical manufacturing industry, we have come across, some of the most wonderful organizations, where innovation is nurtured and encouraged. However, we have not seen many Chandra Siwakoti Sharmas’ at our shop-floor.
We have been some part of several culture change Initiatives, in the pharmaceutical and biological manufacturing organizations, and have seen our share of successes and failures, in the spaces that we have worked. When we look back and ponder on The Most Important Factor for a successful cultural transformation in the organizations, we could not come up with anything else but “the innovative implementation” of a very obvious solution to a herculean, or seeming herculean problem.
Inspired from Mr. Sharma’s tryst with, “no roads” to, “no need of roads” we decided to catalogue our experiences of critical pre-conditions, those need to be present or are required to be developed before a cultural transformation takes place!
While doing so we have taken a case of two similar sized multi-locational pharmaceutical organizations, and who had more or less the same aspirations of cultural transformation. Our time and nature of involvement with both the organizations was also very similar, approximately lasting four months. The work done at both the organizations was more than five years back and thus gives us benefit of assessing the outcome fairly. Needless to say, one organization is a phenomenal success today and other is still, “work in progress”.
We are bound by the confidentiality agreements with both the organizations, and hence will not delve more into the type of work we did with them and the nature and extent of the problem. However, for understanding of the reader of this article, the nature of the problem was, “workforce need to adhere to the standard procedures” or standardization of work processes at shop-floor. For our easy understanding we will name these organizations as “Success” and “work in progress”.
To provide more perspective, both organizations were able to achieve work process standardization at the location/operation, which they were targeting. However, the “success” organization was not only able to transfer the knowledge to other locations, without involving external help, but also was able to improve, on the initial work which was done, to make their processes robust and compliant.
The “work in progress” organization, although were able to achieve their targets then, but were unable to cascade the learning, either from one operation to other similar operations or take the learning into other locations. No further improvements were undertaken by this organization on the work processes. Therefore, it required and still requires constant support to solve similar problems at other locations.
After reading the article on “Jugaad helicopter”, a review of the progress at both the organizations saw the authors spending two months, at the shop-floors of the original manufacturing locations. There were multiple interviews of the shop-floor personnel, managers and senior leadership, across both the organizations. The groups were divided into the following:
1.0 Those who were part of original four-month initiative, a total of 80 shop-floor personnel, 12 managers and 4 leaders.
2.0 Those who joined later in the same department, where original initiative was conducted. A total of 43 shop-floor personnel, 2 managers.
3.0 Other personnel and managers from other departments or locations. A total of 657 shop-floor personnel and 20 managers.
The study also accounted for the attrition in both the organizations; efforts were made to trace and interview the ex-employees; details are depicted in the graph below:
In the following section of this article, we will list and analyze the aspects, those which triggered or hampered, “innovative implementation” at these two organization.
Organization culture, which is conducive of innovation, is characterized with its ability to transform ideas quickly into experiments. These experiments can result in data, which is used for decision making for future change, implemented successfully. This can be divided into following stages:
1.0 Understanding the problem: Significant effort is made to understand the problem/opportunity, before taking next steps, instead of, “knee jerk” action.
2.0 Trust: People are able to experiment with ideas, without fear of backlash.
3.0 Zeal/ Inspiring curiosity: Focus is on What, Why and How, instead of “who”
4.0 Challenge current perspective and not averse to Risk: Processes and perception are put to scientific enquiry, instead of a general attitude of “not rocking the boat”.
5.0 Skill development by fostering partnership: Give and take is deep rooted and employees understand with every, “give” to someone, they are, “taking” a lot of experience.
6.0 Creating freedom and open dialogue: Employees/teams do not wait for right opportunity to speak on issues, rather anyone can discuss their issues, and seek solutions across the length and breadth of the organization.
7.0 Driving discipline/ criticism: Teams/Employees/managers do not feel offended, when feedback is provided, instead seek constructive criticism regularly.
We designed an experiment, to understand the underlying causes of transformation/ or lack of it in both the organizations. Through using tools, the data that emerged is represented below:

As depicted in the graph, the participant from, “success organization” gave higher ratings than, “Work in Progress organization”. This leads to quick implementation of learning, taken by one section/department to the entire organization. The higher ratings in one organization, do indicate a relation between their success and their culture of sustaining “innovative implementation”, when we compare it with the other organization.
However, this brings us to next question, how was one organization able to have all parameters ticked in for sustaining this learnt innovation despite the overall experience, the sizes, scale and challenges of both organizations being similar? We will discuss in the subsequent part of this article….In the meanwhile, if you wish to reach us, please do so at vienni.india@gmail.com.
Contributed by Vishal Sharma



